The surgery of ambulatory patients is totally neglected by doctors in Myanmar. Surgeons who are posted to district and divisional hospitals, practices often as a matter of convenience admit to their hospitals even for minor surgical procedures.
When once in hospital, the patients with minor lesions tend to be lost in the more impressure and dramatic fields of major surgery. So also, general practitioners and younger surgeons who see many of the surgical conditions for which ambulatory care should be given are frequently it prepared to deal with them because of a lack of experience, equipment or assistant.
As medical science advances doctors try to become specialist and according to the march of medical science, the specialists become highly specialized specialist and if that were so who else would be left behind to carry out all the minor ailments of the 95% rural people. Thus ordinary doctor are responsible for minor surgical ailments which is more commonly met daily.
Ambulatory surgery can be carried out easily and safely with limited or adequate equipment and assistance if the surgeon has the gut and mind to perform it. If you have the gut and mind to do it, it is probable that more poor surgery is performed on minor lesions at any time, at any place and at any cost.
If is therefore considered as the work of general practioners and of all the surgeons. It must be remembered that ambulatory surgery has no mortality, requires few assistants and usually can be performed in any place. Eg. In office, out patient department or in any village.
ADVANTAGES OF AMBULATORY SURGERY
-
patient is able to persue his regular occupation with little or no disability.
-
he can go back immediately and stay in his own home, so as to save money which you need to give for his stay in hospitals.
-
because of less worry, the patient do well, and meet no complications,
EQUIPMENT FOR AMBULATORY SURGERY
-
OPERATING ROOM
Operation room is a room with complete or almost completely free of bacteria ( aseptic room ) where surgical procedure is performed.
- to reveal what is not seen or known ( biopsy ).
- to repair bodily disfigurement ( plastic surgery ).
- to amend what is wrong.
- to remove a part, a portion or whole of internal organ which is pathologically damage, to save his life.
- to remove a part, a whole of the extremeties in order to save his/her own life
It could be anywhere so long as it is aseptic in nature and not necessarily be in the so called hospital.
Operating room
- A small room 20 x 20 feet will do.
- Need sufficient light and ventilation.
- Wooden operation table and one or two wooden small table is more than enough.
- One or two, 5 battery torch will substitute for electrical lamp. ( visual surgery – operate against the light ).
- Instead of eclectrical sterilizer boiling method of sterilization will be useful where no electricity is present.
- If no sterilizer drum is available, new cooking pots will do for sterilization of drappers and instruments.
- Bucket, plastic or illumineum for disposal of used water etc.
- Basin one or two for hot water, cleaning of instruments, gauze 6x6 etc. during operation.
- Instruments only essential instruments are need for all surgery the exception of small and few special instruments like badcork, allis forceps, lanes etc. Because surgery is the art of the hand using specially made instruments where hand cannot be used. Eg. You can’t cut the skin or incise the skin with your hand, therefore medical engineers have invented a knife or surgical blades for us so also we cannot hold the small artery or vein with our fingers thus artery forceps or dissecting forceps are made for us, etc.
- bard parker blade holder
dissecting forceps with tooth and without tooth
scissor - pointed and sharp
scissor - curved on flat, Mayo
needle holder – large size, middle size, small size
HAEMOSTAT
Straight and pointed
Straight and curved tip
Mosquito curve
Lane’s tissue forcep
- Suture needles
Straight pointed
Curve rounded 1/2 circle
Curve triangular
Mayo’s round pointed ½ circle
Intestinal of different sizes
- cotton thread No. 20 size and 40 size.
Cat gut 0, 1/0, 2/0, 3/0
- syringes for local ( 20cc, 10cc, 5cc all glass )
- needle for local anesthesia
No.18,21,22,23,25
- bowl for local solution
- draper for different surgical procedure and diseases
- gowns for surgeon
- swabs, gauze rolls, threes etc.
- solution
methylated spirit, tinet iodine
Local anaesthesia
-lignocaine 2%
-burmeton
-phenobarbitone
ANAESTHESIA LOCAL SERVES FOR
-
pain relieving
-
muscular relaxation
-
interfere with nerve conduction
-
success depends upon gaining the confident of the patient
-
surgeon must be gentle and adapt at using local anaesthesia
-
the surgeon must have the thorough knowledge of anatomy. Intelligent use if local anaesthesia is dependent on accurate knowledge of the anatomic relations of nerve trunks to bony landmarks and important surrounding structure.
-
the success of local anaesthesia depends upon gaining the confidence of the patient.
-
there is no special equipment required for local anesthesia.
-
what we need is local anesthetic solution, a bowl, syringes, needles.
-
no special assistant is needed. Whoever near you is your assistant whatever on your table is your instrument.
-
the surgeon administered the local according to his need.
-
consciousness is not lost, various protective body reflexes remain active.
-
recovery from the local effects is rapid, permitting early and safe ambulation.
-
appropriate use of local anesthetic drug has permitted an almost unrestricted variety of surgery to be safely and painlessly performed in ambulatory patients.
TOXICITY OF LOCAL ANESTHETIC SOLUTIONS
Toxicity may result while giving local anesthesia. The early symptoms and signs are as follows.
- dizziness, faintness, yawning
- nausea, vomiting
- shortness of breath
- palpitation
- pallor
- cyanosis
- changes in pulse rate, slower of faster
- sudden fall of blood pressure
- talkativeness excitement followed by fits and convulsions
PRELIMINARY MEDICATION
It is valuable because it relieves fear and anxiety and reduces pain. Most of the surgeons use morphine and pathidine. But it is not wise to use it because it is dangerous and may result asphysia, air hunger etc.
(a) For preliminary medication, I use phenobarbitone sodium in order to decrease nervousness and to counteract the tendency of toxic doses to produce convulsions. ( 200 mg ).
(b) Injection of chlorpheniramine meleate 10mg will prolong the action of lignocaine. The above premedition is used only for major surgery such a thyroidectomy under local block. For others such as lipomas, fibroadenoma breast, piles or haemorrhoids, hydrocoele, hernias etc. The above ( a & b ) is not used.
( A ) LOCAL INFILTRATION ANESTHESIA FOR LIPOMA, SEBAECIOUS CYST, DERMOID
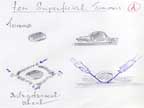 |
Intradermal wheal for incision around the tumor through a primary skin wheal a lone needle is extended with the bevel up along the subcutaneous layer of tissue to a point where the distal intradermal is to be made. An adequate field block satisfies both surgeon and patient. By direct infiltration of the tissues with the anesthetic solution 1%, 2% suitable anesthesia may be obtained for superficial tumors and cysts. If necessary you may also block the base of tumor.
( B ) FOR REDUCTION OF SIMPLE FRACTURES
Direct infiltration of anesthetic solution 1% or 2% into the fracture site i.e into haematoma of fracture will help to reduce the fracture easily without any pain. Therefore anesthesia for the reduction of acute fractures of any of the bones of the extremities may be obtained readily by the direct infiltration of a local anesthetic solution of the fracture site. Thus this is the best method for early fractures reduction.
Combination of local infiltration and nerve block is known as field block. This method will give you a wider zone of anesthesia which usually lasts longer and with smaller quantities of anesthetic solution. A field block type of anesthesia may be preferred to direct local infiltration for removal of sebaceous cysts, lipomas, benign tumors of breast, fibroadenomas and enlarged lymph glands.
The anesthetic solution is injected into the skin and the subcutaneous tissues through an initial skin wheal to form an elliptical or diamond shaped zone of infiltration round the operative field. For cyst and incise injury of lower lip you can remove the cyst or repair the wound of lower lip by injecting 5% 1cc into mental foramen.
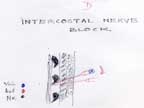
(D) INTERCOSTAL NERVE BLOCK
Intercostal block is used for inserting drainage tube in order to drain the empyema or rib resection. Insert the needle A through an intradermal wheal until you hit or contact the rib. The needle is then slightly withdrawn and reintroduced so that it passes just beneath the lower border of the rib where the three i.e vein, artery, nerve lie in contact for local injection. Inject 1-2cc of local at this point for intercostals block.
( E ) LOCAL BLOCK FOR PERINEUM
Keep the patient in lithotomy position. Inject 1 % 10-20cc of local solution just medial to the ischia tuberocity ( both sites ). This will anesthetise the anterior half of the perineum. With this block you can operate tumors of anterior half of the perineum such as bartholian cyst of the vulve etc. This will anesthetized for labia urethral but not for anus.
( F ) ANAL RING BLOCK FOR PILES
You inject local solution into the anal ring with one finger introducing into the anus and injecting into external& internal anal sphincter to anaesthetized the haemorrhoidal nerves.
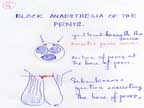
( G ) BLOCK ANAESTHESIA OF THE PENIS
Block anaesthesia of the penis is used for partial ampulation if penis or for phymectomy or meaotomy. The nerves of the penis may be blocked by subcutaneous injection encircleing the base of the penis. The dorsalis penis nerve may also block by injecting 1% - 2% 1cc beneath the fascia.
( H ) DIGITAL NERVE BLOCK FOR OPERATION OF FINGERS AND TOES
The dorsal and volar digital nerves may be blocked within the soft tissues at the base of the fingers or toes.
Raise intradermal wheals on each side, at the base of the finger or toe.
Then introduce the needle through these intradermal wheals into deeper tissues.
Inject 1cc of 1% lignocaine close to the bone to anaesthetized the anterior and posterior digital nerves. i.e. dorsal and volar nerves.
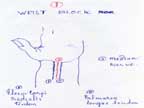
( I ) MEDIAN, RADIAL, ULNAR NERVE BLOCK
Operations on the hand for crushed injury or finger amputation could be performed by a block of the sensory nerves at the wrist.
If not effective you may add subcutaneous bracelet infiltration about the wrist.
For the success of this block you must have a fairly good knowledge of the locations of the main nerve trucks, so as to inject the solution actually into the nerve trunk or close to it.
The median nerve is superficial in the wrist and lies directly beneath and between the tendons of the palmaris longus and flexor carpi radalis.
Inject or insert a needle through an intradermal wheal deep into in between the palmaris longus tendon and flexor carpiradialis tendon.
Paresthesias will be obtained in the thumb or the index finger.
Then inject 1% 1-2cc of local anesthesia. So as to get median nerve block.The ulnar nerve lies just to the radial side of the flexor carpi ulnaris which serves as a landmark in the block of ulnar nerve.
(J) ULNAR NERVE BLOCK
Ulnar nerve block could be easily performed at the elbow as the nerve is very much superficial and could be felt as a round cord in the medial olecranon groove.
Inject directly into the groove with 1% 1-2cc of local for block.
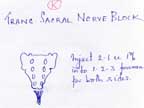
Caudal anaesthesia or trans sacrak block is to block the 3rd , 4th and 5th sacral nerves. Block of these sacral nerves roots by injectiog 1% 5cc of local into the sacral canal produces anaesthesia of the structures of the perineum and the external genitalia which is adequate for perineal surgery of the genitor urinary tract for anorectal surgery and for minor gynecological procedures.
For transsacral block, imaginary line is drawn from one posterior superior iliac spine to the opposite posterior superior iliac spine. A finger breath downward or below this imaginary line lies right and left sacral foramena. A finger breath from an imaginary median line outward will give you the site of foramens.
As an ambulatory surgeon during my service of 1965-2005 I according to my motto – to teach, to preach and to heal, I used to tour to visit almost all of the villages within my jurisdiction with the missionary zeal and spirit to study the way of their life and their health status.
I have collected the population census of their village and give talk of health how to live as a healthy people. I also examined them for lumps and bumps and phymosis, hernia, lipoma, cysts, fibroadenoma breast, prolapses, hydrocele, hare lip etc.
Then having made the first and after given health education for its dangers and complications with photos of different diseases that I have recorded. I try to persuade and perform ambulatory surgery for phymosis, breast tumors, fibroadenoma breast, inguinal hernias and hydrocoele etc. under local analgesia. At the same time for major surgery I invited them to come to my hospital for free surgery. Thus, by such performance I become a local ambulatory surgeon in that locality.
With such zeal and spirit and with difficulty I have to go to the remote areas unserveyed area of Myanmar - India border the so called Naga Land ( 1965-1971 ).
The governing authorities under General Ne Win and the then Health Minister Colonel Hla Han gave me a full support offered 40 mules for my travel and to carry my equipment and medicines for there is no communication to travel with car or any vehicles what so ever.
In case of necessity drugs and utensils are dropped down for me by airforce parachutes.
But so sorry to mention there was not a single doctor or a nurse to give a helping hand for my tour and surgical performances. Doctors and nurses are reluctant to visit and stay with me for this job.
Anyhow, my believe and faith of human beings i.e all human beings are equal and alike, they are the statue of God and they are the highest in the animal kingdom known as two legged creature is true.
So also surgery being art of the hand and thus due to unavoidable circumstances, I have to perform my field surgery within their house or outside in the open air operation theatre without any facility.
Anybody near me is my assistant thus I ask the people who are witnesting my surgery who will be my assistant to help me.
Also by practicing myself to have the four essence of a surgeon, i.e heart of a lion, hands of a lady, eyes of an eagle and mouth of an angel. I become a good field surgeon who could perform all minor surgery without assistant doctor or nurse, without facility anywhere at any time.
Even in the hospitals I used to operate all the major cases by spinal ( low, middle, high ) for abdominal cases such as G&GJ with high spinal, Intestinal obstruction, appendicitis etc. with middle spinal and gynaecological surgery by lower spinal . Even Ceacerian Section by local infiltration block combined with pelvic block etc.
Only for exploratory laprotomy I use General Aneasthesia.
Basing on my theories and techniques which I have read from many books, I try to do all of the surgical procedure under local anaesthetic block and it become very successful.
THE CONSEQUENCES WHO FAIL TO FOLLOW THE 5 DON’TS
- Do not touch unnecessarily.
- Do not press or exert pressure or do not massage
- Do not apply ointments or herbs.
- Do not puncture or inject or aspirate.
- Do not take unnecessarily drug without knowing the cause.
These 5 don’ts prevent complications.
Lumps, bumps ie. Tomour external or internal no matter where the site is, the result or cause of it is not infection, therefore no other treatment except surgical removal.
If fail to follow my advice you will really face complications. To have confidence and belief I show them complicated case due to frequent touch, frequent massage, due to application of herbal ointments and due to acute puncture.
Mass phymectomy is also carried out in my township to prevent carcinoma penis.
Showing the stages of Ca Penis.
Therefore as an ambulatory touring surgeon during my 1962 – 2002 period of 40 years have carried out the 5 essence or duties of a doctor. i.e
To prevent
To educate
To relief their suffering
To do minor research and
To rehabilitate them.
As a pioneer and like a missionary doctor with missionary zeal and spirit my work of ambulatory surgeon is highly honored and remembered by the rural people of the remote places in Myanmar.
This is to mention and reveal in this series of my work is to initiate the younger doctors to follow and continue a lot of minor ailments and minor surgery for the rural people who are much neglected by our doctors of the past and the present.
Wish you to be like me
Thank you.
|